

Health Library
Myelomeningocele
Meningomyelocele; Spina bifida; Cleft spine; Neural tube defect (NTD); Birth defect - myelomeningocele
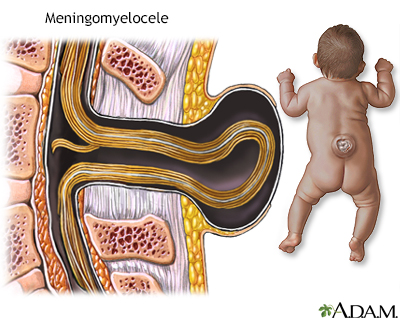
Myelomeningocele is a birth defect in which the backbone and spinal canal do not close fully before birth.
The condition is a type of neural tube defect (NTD).
Images
I Would Like to Learn About:
Causes
During the first month of a pregnancy, the two sides of the baby's spine (or backbone) usually join together to cover the spinal cord, spinal nerves, and meninges (the tissues covering the spinal cord). The developing brain and spine at this point are called the neural tube. The term "NTD" refers to any birth defect in which the neural tube in the area of the spine fails to close completely.
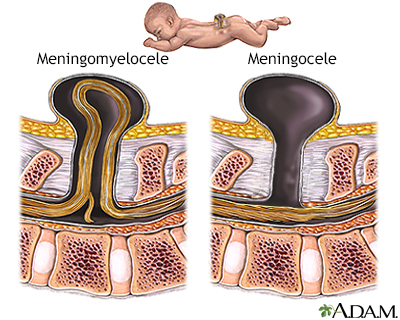
Myelomeningocele is an NTD in which the bones of the spine do not completely form. This results in an incomplete spinal canal. The spinal cord and meninges protrude from the child's back.
This condition may affect as many as 1 out of every 3,000 infants.
Other types of NTDs include:
- Spina bifida occulta, a condition in which the bones of the spine do not close. The spinal cord and meninges remain in place and skin usually covers the defect.
- Meningoceles, a condition in which the meninges protrude from the spinal defect. The spinal cord remains in place.
- Encephaloceles, a condition in which the meninges and even brain can protrude from the skull.
A child with myelomeningocele may also have other disorders or birth defects. Eight out of ten children with this condition have hydrocephalus, or an abnormal buildup of spinal fluid in the ventricles of the brain.
Other disorders of the spinal cord or musculoskeletal system may be seen with myelomeningocele, including:
- Syringomyelia (a fluid-filled cyst within the spinal cord)
- Hip dislocation
The cause of NTDs is not known. However, low levels of folic acid in a woman's body before and during early pregnancy appear to play a part in this type of birth defect. Folic acid (or folate) is important for development of brain and spinal cord.
If a child is born with a myelomeningocele, future children in that family have a higher risk than the general population. However, in many cases, there is no family connection. Factors such as diabetes, obesity, and the use of anti-seizure and other medicines known to lower folic acid levels in the mother may increase the risk of this defect.
Symptoms
A newborn with this disorder will have an open area or a fluid-filled sac on the mid to lower back.
Symptoms may include:
- Loss of bladder or bowel control
- Partial or complete lack of sensation
- Partial or complete paralysis of the legs
- Weakness of the hips, legs, or feet of a newborn
Other signs and/or symptoms may include:
- Abnormal feet or legs, such as clubfoot
- Buildup of fluid inside the skull (hydrocephalus)
Exams and Tests
Prenatal screening can help detect this condition. During the second trimester, pregnant women can have a blood test called the quadruple screen test. This test screens for myelomeningocele, Down syndrome, and other congenital diseases in the baby. Most women carrying a baby with spina bifida will have an increased level of a protein called maternal alpha fetoprotein (AFP).
If the quadruple screen test is positive, further testing is needed to confirm the diagnosis.
Such tests may include:
Myelomeningocele can be seen after the child is born. A neurologic exam may show that the child has loss of nerve-related functions below the defect. For example, watching how the infant responds to pinpricks at various locations may tell where the baby can feel the sensations.
Tests done on the baby after birth may include x-rays, ultrasound, CT, or MRI of the spinal area.
Treatment
The health care provider may suggest genetic counseling. Intrauterine surgery to close the defect (before the baby is born) may reduce the risk of some later complications.
After your baby is born, surgery to repair the defect is most often suggested within the first few days of life. Outcomes are better if the birth takes place in a center where the repair can be done. Before surgery, your baby must be handled carefully to reduce damage to the exposed spinal cord. This may include:
- Special care and positioning
- Protective devices
- Changes in the methods of handling, feeding, and bathing
Children who also have hydrocephalus may need to have a ventriculoperitoneal shunt placed. This will help drain the extra fluid from the ventricles (in the brain) to the peritoneal cavity (in the abdomen).
Antibiotics may be used to treat or prevent infections such as meningitis or urinary tract infections.
Most children will need lifelong treatment for problems that result from damage to the spinal cord and spinal nerves.
This includes:
- Bladder and bowel problems -- Gentle downward pressure over the bladder may help drain the bladder. Drainage tubes, called catheters, may be needed as well. Bowel training programs and a high fiber diet may improve bowel function.
- Muscle and joint problems -- Orthopedic or physical therapy may be needed to treat musculoskeletal symptoms. Braces may be needed. Many people with myelomeningocele primarily use a wheelchair.
Follow-up exams generally continue throughout the child's life. These are done to:
- Check developmental progress
- Treat any intellectual, neurological, or physical problems
Visiting nurses, social services, support groups, and local agencies can provide emotional support and assist with the care of a child with a myelomeningocele who has significant problems or limitations.
Support Groups
Taking part in a spina bifida support group may be helpful for families.
Outlook (Prognosis)
A myelomeningocele can most often be surgically corrected, but the affected nerves may still not function normally. The higher the location of the defect on the baby's back, the more nerves will be affected.
With early treatment, length of life is not severely affected. Kidney problems due to poor drainage of urine are the most common cause of death.
Most children will have normal intelligence. However, because of the risk of hydrocephalus and meningitis, more of these children will have learning problems and seizure disorders than the general population.
New problems within the spinal cord can develop later in life, especially after the child begins growing rapidly during puberty. This can lead to more loss of function as well as orthopedic problems such as scoliosis, foot or ankle deformities, dislocated hips, and joint tightness or contractures.
Many people with myelomeningocele primarily use a wheelchair.
Possible Complications
Complications of spina bifida may include:
- Traumatic birth and difficult delivery of the baby
- Frequent urinary tract infections
- Fluid buildup on the brain (hydrocephalus)
- Loss of bowel or bladder control
- Brain infection (meningitis)
- Permanent weakness or paralysis of legs
This list may not be all-inclusive.
When to Contact a Medical Professional
Contact your child's provider if:
- A sac or open area is visible on the spine of a newborn infant
- Your child is late in walking or crawling
- Symptoms of hydrocephalus develop, including bulging soft spot, irritability, extreme sleepiness, and feeding difficulties
- Symptoms of meningitis develop, including fever, stiff neck, irritability, and a high-pitched cry
Prevention
Folic acid supplements may help reduce the risk of neural tube defects such as myelomeningocele. It is recommended that any woman considering becoming pregnant take 0.4 mg of folic acid a day. Pregnant women with high risk need a higher dosage.
It is important to remember that folic acid deficiencies must be corrected before becoming pregnant, because the defects develop very early.
Women who plan to become pregnant may be screened to determine the amount of folic acid in their blood.
Related Information
Central nervous systemFolate deficiency
Muscle function loss
Numbness and tingling
Urinary incontinence
Meningitis
Hydrocephalus
Syringomyelia
Dislocation
Cerebral palsy
Ventriculoperitoneal shunt - discharge
References
Committee Opinion No. 720: Maternal-Fetal Surgery for Myelomeningocele. Obstet Gynecol. 2017;130(3):e164-e167. PMID: 28832491 pubmed.ncbi.nlm.nih.gov/28832491/.
Licci M, Guzman R, Soleman J. Maternal and obstetric complications in fetal surgery for prenatal myelomeningocele repair: a systematic review. Neurosurg Focus. 2019;47(4):E11. PMID: 31574465 pubmed.ncbi.nlm.nih.gov/31574465/.
Trowbridge SK, Yang E, Yuskaitis CJ. Congenital anomalies of the central nervous system. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 631.
Wilson PE, Simpson TS. Meningomyelocele (spina bifida). In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 754.
BACK TO TOPReview Date: 10/3/2025
Reviewed By: Mary Terrell, MD, NABBLM-C, IBCLC, Neonatologist, Cape Fear Valley Medical Center, Fayetteville, NC. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language.
© 1997-
2026 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures.
![]()