

Health Library
Transient ischemic attack
Mini stroke; TIA; Little stroke; Cerebrovascular disease - TIA; Carotid artery - TIA
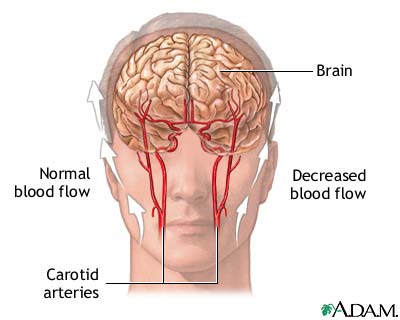
A transient ischemic attack (TIA) occurs when blood flow to a part of the brain stops for a brief time. A person will have stroke-like symptoms for up to 24 hours. In most cases, the symptoms last for 1 to 2 hours.
A transient ischemic attack is a warning sign that a true stroke may happen in the future (often near future) if something is not done to prevent it.
Images

I Would Like to Learn About:
Causes
A TIA is different than a stroke. After a TIA, the blockage breaks up quickly and dissolves on its own. A TIA does not cause brain tissue to die.
The loss of blood flow to an area of the brain can be caused by:
- A blood clot in an artery of the brain
- A blood clot that travels to the brain from somewhere else in the body (for example, from the heart)
- An injury to blood vessels
- Narrowing of a blood vessel in the brain or leading to the brain
High blood pressure is the main risk factor for TIAs and stroke. Other major risk factors are:
- Irregular heartbeat called atrial fibrillation
- Diabetes
- Family history of stroke
- Being male
- High cholesterol
- Tendency to have abnormal blood clotting
- Increasing age, especially after age 55
- Ethnicity (African Americans are more likely to die of stroke)
- Smoking
- Alcohol use
- Recreational drug use
- History of prior TIA or stroke
People who have heart disease or poor blood flow in their legs caused by narrowed arteries are also more likely to have a TIA or stroke.
Symptoms
Symptoms begin suddenly, last a short time (from a few minutes to 1 to 2 hours), and go away. They may occur again at a later time.
The symptoms of a TIA are the same as the symptoms of a stroke, and include:
- Change in alertness (including sleepiness or unconsciousness)
- Changes in the senses (such as hearing, vision, taste, and touch)
- Mental changes (such as confusion, memory loss, difficulty writing or reading, trouble speaking or understanding others)
- Muscle problems (such as weakness, trouble swallowing, trouble walking)
- Dizziness or loss of balance and coordination
- Lack of control over the bladder or bowels
- Sensation problems (such as numbness or tingling on one side of the body)
Exams and Tests
While the symptoms and signs of a TIA may go away by the time you get to the hospital, it is important to be evaluated right away. In the event your symptoms don't go away, all treatments are more effective the sooner they are given. Someone with a TIA is also very likely to have a stroke in the following days to weeks. A TIA diagnosis may be made based on your medical history alone.
Your health care provider will do a complete physical exam to check for heart and blood vessel problems. You will also be checked for nerve and muscle problems.
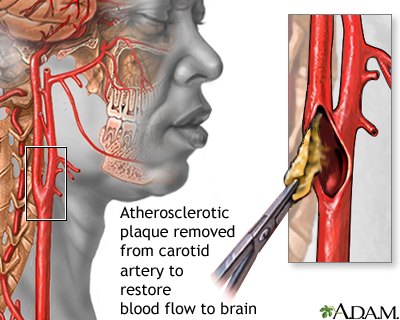
Your provider will use a stethoscope to listen to your heart and arteries. An abnormal sound called a bruit may be heard when listening to the carotid artery in your neck or other artery. A bruit is caused by irregular blood flow.
Tests will be done to check for a stroke or other disorders that may cause the symptoms:
- You will likely have a head CT scan or brain MRI. A stroke may show changes on these tests, but TIAs will not.
- You may have an angiogram, CT angiogram, or MR angiogram to see which blood vessel is blocked or bleeding.
- You may have an echocardiogram if your provider thinks you may have a blood clot from the heart.
- You may have a carotid duplex ultrasound. It can show if the carotid arteries in your neck have narrowed.
- You will likely have an electrocardiogram (ECG) and heart rhythm monitoring tests to check for an irregular heartbeat.
Your provider may do other tests to check for high blood pressure, heart disease including an irregular heartbeat, diabetes, high cholesterol, and other causes of, and risk factors for TIAs or stroke. You may have an EEG test to check if your symptoms are not due to a seizure.
Treatment
If you have had a TIA within the last 48 hours, you will likely be admitted to the hospital so that your providers can search for the cause and monitor you.
High blood pressure, heart disease, diabetes, high cholesterol, and blood disorders will be treated as needed. You will be encouraged to make lifestyle changes to reduce your risk of further symptoms. Changes include quitting smoking, exercising more, and eating healthier foods.
You may receive blood thinners, such as aspirin, heparin, warfarin, or direct acting oral anticoagulants (DOACs) to reduce blood clotting. Some people who have blocked neck arteries may need surgery (carotid endarterectomy). If you have an irregular heartbeat (atrial fibrillation) or other heart problems, you will be treated to avoid future complications.
Outlook (Prognosis)
TIAs do not cause lasting damage to the brain.
But, TIAs are a warning sign that you may have a true stroke in the coming days or months. Some people who have a TIA will have a stroke within 3 months. Half of these strokes happen during the 48 hours after a TIA. The stroke may occur that same day or at a later time. Some people have only a single TIA, and others have more than one TIA.
You can reduce your chances of a future stroke by following up with your provider to manage your risk factors.
When to Contact a Medical Professional
A TIA is a medical emergency. Call 911 or the local emergency number right away. Do not ignore symptoms just because they go away. They may be a warning of a future stroke.
Prevention
Follow your provider's instructions on how to prevent TIAs and strokes. You will likely be told to make lifestyle changes and take medicines to treat high blood pressure or high cholesterol.
Related Information
Carotid artery surgery - openCarotid artery disease
Recovering after stroke
Angioplasty and stent placement - carotid artery - discharge
Atrial fibrillation - discharge
Carotid artery surgery - discharge
Taking warfarin
Stroke - discharge
References
Biller J, Ruland S, Schneck MJ. Ischemic cerebrovascular disease. In Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. Philadelphia, PA: Elsevier; 2022:chap 65.
Bushnell C, Kernan WN, Sharrief AZ, et al. 2024 Guideline for the primary prevention of stroke: A guideline from the American Heart Association/American Stroke Association. Stroke. 2024;55(12):e344-e424. PMID: 39429201 pubmed.ncbi.nlm.nih.gov/39429201/.
Chaturvedi S, Selim M. Hemorrhagic cerebrovascular disease. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 377.
Gladstone DJ, Lindsay MP, Douketis J, et al. Canadian stroke consortium. Canadian stroke best practice recommendations: secondary prevention of stroke Update 2020. Can J Neurol Sci. 2022;49(3):315-337. PMID: 34140063 pubmed.ncbi.nlm.nih.gov/34140063/.
Goldstein LB. Ischemic cerebrovascular disease. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 376.
Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149(1):e1-e156. PMID: 38033089 pmc.ncbi.nlm.nih.gov/articles/PMC11095842/.
Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021;52(7):e364-e467. PMID: 34024117 pubmed.ncbi.nlm.nih.gov/34024117/.
Papa L, Meurer WJ. Stroke. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 87.
Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. PMID: 31662037 pubmed.ncbi.nlm.nih.gov/31662037/.
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;72(3):e127-e248. PMID: 29133354 pubmed.ncbi.nlm.nih.gov/29133354/.
BACK TO TOPReview Date: 4/16/2025
Reviewed By: Joseph V. Campellone, MD, Department of Neurology, Cooper Medical School at Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language.
© 1997-
2026 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures.
![]()