

Calcium pyrophosphate arthritis
Calcium pyrophosphate dihydrate deposition disease; CPPD disease; Acute/chronic CPPD arthritis; Pseudogout; Pyrophosphate arthropathy; Chondrocalcinosis
Calcium pyrophosphate dihydrate (CPPD) arthritis is a joint disease that can cause attacks of arthritis. Like gout, crystals form in the joints. But in this kind of arthritis, the crystals are not formed from uric acid.

Causes
Deposition of calcium pyrophosphate dihydrate (CPPD) causes this form of arthritis. The buildup of this chemical forms crystals in the cartilage of joints. This leads to attacks of joint swelling and pain most often in the knees, wrists, ankles, and shoulders. Other joints can be affected as well. In contrast to gout, the metatarsal-phalangeal joint of the big toe is not often affected.


Among older adults, CPPD is a common cause of sudden (acute) arthritis in one joint. The attack may be caused by:
- Injury to the joint
- Medical stress
CPPD arthritis mainly affects the elderly because joint degeneration and osteoarthritis increases with age. Such joint damage increases the tendency of CPPD deposition. However, CPPD arthritis is also more common in people with:

- Hemochromatosis
- Parathyroid gland disease
- Dialysis-dependent renal failure

Symptoms
In most cases, CPPD deposits do not cause any symptoms. Instead, x-rays of affected joints such as knees show characteristic deposits of calcium. This is called chondrocalcinosis.
Some people with chronic CPPD deposits in large joints may have the following symptoms:
- Pain
- Swelling
- Warmth
- Redness
Attacks of joint pain can last for months. There may be no symptoms between attacks.
In some people CPPD arthritis causes severe damage to a joint.
CPPD arthritis can also occur in the upper and lower spine. Pressure on spinal nerves may cause pain in the arms or legs.
Because the symptoms are similar, CPPD arthritis can be confused with:
- Gouty arthritis (gout)
- Osteoarthritis
- Rheumatoid arthritis

Exams and Tests
Most arthritic conditions show similar symptoms. Carefully testing the joint fluid for crystals can help the health care provider diagnose the condition.
You may have the following tests:
- Joint fluid exam to detect white blood cells and calcium pyrophosphate crystals
- Joint x-rays to look for joint damage and calcium deposits in joint spaces
- Other joint imaging tests such as CT scan, MRI or ultrasound, if required
- Blood tests to screen for conditions that are linked to calcium pyrophosphate arthritis

Treatment
Treatment may involve removing fluid to relieve pressure in the joint. A needle is placed into the joint and fluid is removed. Some common treatment options are:
- Steroid injections to treat severely swollen joints
- Oral steroids to treat multiple swollen joints
- Nonsteroidal anti-inflammatory medicines (NSAIDs) to ease the pain
- Colchicine to treat attacks of CPPD arthritis
- For chronic CPPD arthritis in multiple joints, methotrexate or hydroxychloroquine may be helpful
Outlook (Prognosis)
Most people do well with treatment to reduce the acute joint pain. A medicine such as colchicine may help prevent repeat attacks. There is no treatment to remove the CPPD crystals.
Possible Complications
Permanent joint damage can occur without treatment.
When to Contact a Medical Professional
Contact your provider if you have attacks of joint swelling and joint pain.
Prevention
There is no known way to prevent this disorder. However, treating other problems that may cause CPPD arthritis may make the condition less severe.
Regular follow-up visits may help prevent permanent damage of the affected joints.
References
Edwards NL. Crystal deposition diseases. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 252.
Rosenthal AK, Tedeschi SK, Mccarthy GM, Cowley S. Calcium crystal disease: calcium pyrophosphate deposition disease and basic calcium phosphate-associated syndromes. In: Firestein GS, McInnes IB, Koretzky GA, Mikuls TR, Neogi T, O'Dell JR, eds. Firestein & Kelley's Textbook of Rheumatology. 12th ed. Philadelphia, PA: Elsevier; 2025:chap 98.
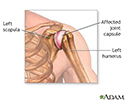
Shoulder joint inflammation - illustration
Shoulder joint inflammation
illustration
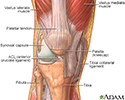
The structure of a joint - illustration
The structure of a joint
illustration
Review Date: 1/16/2026
Reviewed By: Diane M. Horowitz, MD, Rheumatology and Internal Medicine, Northwell Health, Great Neck, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
© 1997- A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.