

Health Library
Mastectomy
Breast removal surgery; Subcutaneous mastectomy; Nipple sparing mastectomy; Total mastectomy; Skin sparing mastectomy; Simple mastectomy; Modified radical mastectomy; Breast cancer - mastectomy; Prophylactic mastectomy; Risk reduction mastectomy
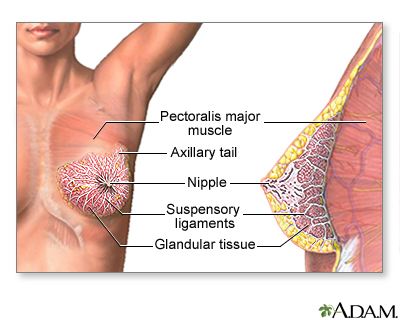
A mastectomy is surgery to remove the breast tissue. Some of the skin and the nipple may also be removed. The surgery is most often done to treat breast cancer.
Images
Presentation


I Would Like to Learn About:
Description
Before surgery begins, you will be given general anesthesia. This means you will be asleep and pain-free during surgery.
There are different types of mastectomies. Which one your surgeon performs depends on the type of breast problem you have. Most of the time, a mastectomy is done to treat breast cancer. However, it is sometimes done to prevent cancer (prophylactic mastectomy).
The surgeon will make a cut in your breast and perform one of these operations:
- Nipple-sparing mastectomy: The surgeon removes your entire breast, but leaves the nipple and areola (the colored circle around the nipple) in place. If you have cancer, the surgeon may do a biopsy of lymph nodes in the underarm area to see if the cancer has spread.
- Skin-sparing mastectomy: The surgeon removes your breast with the nipple and areola with minimal skin removal. If you have cancer, the surgeon may do a biopsy of lymph nodes in the underarm area to see if the cancer has spread.
- Total or simple mastectomy: The surgeon removes your entire breast along with the nipple and areola. If you have cancer, the surgeon may do a biopsy of lymph nodes in the underarm area to see if the cancer has spread.
- Modified radical mastectomy: The surgeon removes your entire breast with the nipple and areolar along with some of the lymph nodes underneath the arm.
- Radical mastectomy: The surgeon removes your entire breast with the nipple and areola along with the skin over your breast, all of the lymph nodes underneath the arm, and the skin is then closed with sutures (stitches).
One or two small plastic drains or tubes are very often left in your chest to remove extra fluid from where the breast tissue used to be.
A plastic surgeon may be able to begin reconstruction of your breast during the same operation. You may also choose to have breast reconstruction at a later time. If you have reconstruction, a skin- or nipple-sparing mastectomy may be an option.
A mastectomy will take about 2 to 3 hours.
Why the Procedure Is Performed
WOMEN DIAGNOSED WITH BREAST CANCER
The most common reason for a mastectomy is breast cancer.
If you are diagnosed with breast cancer, talk to your health care provider about your choices:
- Lumpectomy is when only the breast cancer and tissue around the cancer are removed. This is also called breast conservation therapy or partial mastectomy. Most of your breast will be left.
- Mastectomy is when all breast tissue is removed.
You and your provider should consider:
- The size and location of your tumor
- Skin involvement of the tumor
- How many tumors there are in your breast
- How much of your breast is affected
- The size of your breast
- Your age
- Medical history that may exclude you from breast conservation (this may include prior breast radiation and certain medical conditions)
- Family history
- Your general health and whether you have reached menopause
You and your providers who are treating your breast cancer will decide together which option is right for you.
WOMEN AT HIGH RISK FOR BREAST CANCER
Women who have a very high risk of developing breast cancer may choose to have a preventive (or prophylactic) mastectomy to reduce the risk of breast cancer.
You may be more likely to get breast cancer if one or more close family relatives has had the disease, especially at an early age. Genetic tests (such as BRCA1 or BRCA2) may help show that you have a high risk. However, even with a normal genetic test, you may still be at high risk for breast cancer, depending on other factors. It may be useful to meet with a genetic counselor to assess your level of risk.
A prophylactic mastectomy should be done only after very careful thought and discussion with your doctor, a genetic counselor, your family, and loved ones.
A mastectomy greatly reduces the risk for breast cancer, but does not eliminate it.
You may decide to have a mastectomy based on your personal preference for a given condition. You and your provider will discuss the pros and cons of this decision.
Risks
Scabbing, blistering, wound opening, bleeding, seroma, or skin loss along the edge of the surgical cut or within the skin flaps may occur.
Risks:
- Shoulder pain and stiffness. You may also feel pins and needles where your breast used to be and underneath the arm.
- Swelling of your arm (called lymphedema) on the same side as your breast that is removed. This swelling is not common, but it can be an ongoing problem.
- Damage to nerves that go to the muscles of the arm, back, and chest wall.
- Loss of sensation of the skin of your chest wall.
Before the Procedure
You may have blood and imaging tests (such as CT scan, bone scan, PET scan) after your provider finds breast cancer. This is done to determine if the cancer has spread outside of the breast and lymph nodes under the arm. These tests are not needed if you have early stage breast cancer.
Tell your surgeon or nurse if:
- You are or could be pregnant
- You are taking any medicines, including medicines, drugs, supplements, or herbs you bought without a prescription.
Planning for your surgery:
- If you have diabetes, heart disease, or other medical conditions, your surgeon may ask you to see your provider who treats you for these conditions.
- If you smoke, it's important to cut back or quit. Smoking can slow healing and increase the risk for blood clots. Ask your provider for help quitting smoking.
- If needed, prepare your home to make it easier to recover after surgery.
- Ask your surgeon if you need to arrange to have someone drive you home after your surgery
During the week before your surgery:
- You may be asked to temporarily stop taking medicines that keep your blood from clotting. These medicines are called blood thinners. This includes over-the-counter medicines and supplements such as aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), and vitamin E. Many prescription medicines are also blood thinners.
- Ask your surgeon which medicines you should still take on the day of surgery.
- Let your surgeon know about any illness you may have before your surgery. This includes COVID-19, cold, flu, fever, herpes breakout, or other illness. If you do get sick, your surgery may need to be postponed
On the day of the surgery:
- Follow instructions about when to stop eating and drinking..
- Take the medicines your surgeon told you to take with a small sip of water.
- Follow instructions on when to arrive at the hospital. Be sure to arrive on time
After the Procedure
Most women stay in the hospital for 24 hours after a mastectomy, though some women may be able to go home the day of surgery. Your length of stay will depend on the type of surgery you had. Many women go home with drainage tubes still in their chest after mastectomy. The drains will be removed later during an office visit with your surgeon. A nurse will teach you how to look after the drain, or you might be able to have a home care nurse help you.
You may have pain around the site of your cut after surgery. The pain is worst in the first few days after surgery and then goes away over a period of several weeks. You will receive pain medicines during your hospital stay. Talk with your surgeon about medicines to take for pain after surgery.
Fluid may collect in the area of your mastectomy after all the drains are removed. This is called a seroma. It most often goes away on its own, but it may need to be drained using a needle (aspiration).
Outlook (Prognosis)
Most women recover well after mastectomy.
In addition to surgery, you may need other treatments for breast cancer. If hormonal therapy or chemotherapy are indicated, you will meet with a medical oncologist. If radiation therapy is recommended, you will meet with a radiation oncologist.
Related Information
Breast cancerBreast lump removal
Radiation therapy
Breast reconstruction - implants
Breast reconstruction - natural tissue
Lymphedema - self-care
Breast external beam radiation - discharge
After chemotherapy - discharge
Dry mouth during cancer treatment
Eating extra calories when sick - adults
Surgical wound care - open
Oral mucositis - self-care
Chest radiation - discharge
Drinking water safely during cancer treatment
Safe eating during cancer treatment
Mastectomy - discharge
Mastectomy and breast reconstruction - what to ask your doctor
Cosmetic breast surgery - discharge
References
Davidson NE. Breast cancer and benign breast disorders. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 183.
Gradishar WJ, Moran MS, Abraham J, et al. Breast cancer, version 3.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2024;22(5):331-357. PMID: 39019058 pubmed.ncbi.nlm.nih.gov/39019058/.
Henry NL, Shah PD, Haider I, Freer PE, Jagsi R, Sabel MS. Cancer of the breast. In: Niederhuber JE, Armitage JO, Kastan MB, Doroshow JH, Tepper JE, eds. Abeloff's Clinical Oncology. 6th ed. Philadelphia, PA: Elsevier; 2020:chap 88.
Klimberg VS, Hunt KH. Diseases of the breast. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 35.
Macmillan RD. Mastectomy. In: Dixon JM, Barber MD, eds. Breast Surgery: A Companion to Specialist Surgical Practice. 7th ed. Philadelphia, PA: Elsevier; 2024:112-121.
BACK TO TOPReview Date: 2/17/2025
Reviewed By: David A. Lickstein, MD, FACS, specializing in cosmetic and reconstructive plastic surgery, Palm Beach Gardens, FL. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
![]()