

Health Library
Growth hormone deficiency - children
Pituitary dwarfism; Acquired growth hormone deficiency; Isolated growth hormone deficiency; Congenital growth hormone deficiency; Panhypopituitarism; Short stature - growth hormone deficiency
Growth hormone deficiency means the pituitary gland does not make enough growth hormone.
Images

I Would Like to Learn About:
Causes
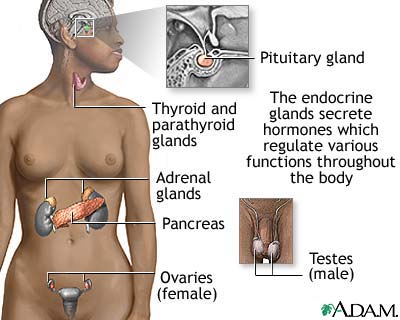
The pituitary gland is located at the base of the brain. This gland controls the body's balance of hormones. It also makes growth hormone. This hormone causes a child to grow.
Growth hormone deficiency may be present at birth. Growth hormone deficiency may be the result of a medical condition. Severe brain injury may also cause growth hormone deficiency.
Children with physical defects of the face and skull, such as cleft lip or cleft palate, may have decreased growth hormone level.
Most of the time, the cause of growth hormone deficiency is unknown.
Symptoms
Slow growth may first be noticed in infancy and continue through childhood. Your child's health care provider will most often draw your child's growth curve on a growth chart. Children with growth hormone deficiency have a slow or flat rate of growth. The slow growth may not show up until a child is 2 or 3 years old.
The child will be much shorter than most children of the same age and sex. The child will still have normal body proportions, but may be chubby. The child's face often looks younger than other children of the same age. The child will have normal intelligence in most cases.
In older children, puberty may come late or may not come at all, depending on the cause.
Exams and Tests
A physical exam, including weight, height, and body proportions, will show signs of slowed growth. The child will not follow the normal growth curves.
A hand x-ray can determine bone age. Normally, the size and shape of bones change as a person grows. These changes can be seen on an x-ray and they most often follow a pattern as a child grows older.
Testing is most often done after your child's provider has looked into other causes of poor growth. Tests that may be done include:
- Insulin-like growth factor 1 (IGF-1) and insulin-like growth factor binding protein 3 (IGFBP3). These are substances that growth hormone cause the body to make. Tests can measure these growth factors. Accurate growth hormone deficiency testing involves a stimulation test. This test takes several hours.
- MRI of the head can show the hypothalamus and pituitary glands.
- Tests to measure other hormone levels may be done, because a lack of growth hormone may not be the only problem.
Treatment
Treatment involves growth hormone shots (injections) given at home. The shots are most often given once a day. Older children can often learn how to give themselves the shot.
Treatment with growth hormone is long-term, often lasting for several years. During this time, your child needs to be seen regularly by their provider to ensure the treatment is working. If needed, your child's provider will change the dosage of the medicine.
Serious side effects of growth hormone treatment are rare. Common side effects include:
- Headache
- Fluid retention
- Muscle and joint aches
- Slippage of the hip bones
Outlook (Prognosis)
The earlier the condition is treated, the better the chance that your child will grow to near-normal adult height. Many children gain 4 or more inches (in) or about 10 centimeters (cm) during the first year, and 3 or more inches (about 7.6 cm) during the next 2 years. The rate of growth then slowly decreases.
Growth hormone therapy does not work for all children.
Left untreated, growth hormone deficiency may lead to short stature and delayed puberty.
Growth hormone deficiency can occur with deficiencies of other hormones such as those that control:
- Production of thyroid hormones
- Water balance in the body
- Production of male and female sex hormones
- The adrenal glands and their production of cortisol, DHEA, and other hormones
When to Contact a Medical Professional
Contact your child's provider if they seem abnormally short for their age.
Prevention
Most cases are not preventable.
Review your child's growth chart with your child's provider at each checkup. If there is concern about your child's growth rate, evaluation by a specialist is recommended.
Related Information
Short statureGrowth hormone test
Hormone levels
Antidiuretic hormone blood test
ACTH blood test
Adrenal glands
Creutzfeldt-Jakob disease
References
Dattani MT, Dastamani A. Growth hormone deficiency in children. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 18.
Divall SA, Radovick S. Normal and aberrant growth in children. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15th ed. Philadelphia, PA: Elsevier; 2025:chap 22.
Patterson BC, Felner EI. Hypopituitarism. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 595.
Weiss RE. Anterior pituitary. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 205.
BACK TO TOPReview Date: 7/1/2025
Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language.
© 1997-
2026 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures.
![]()