

Health Library
Primary amyloidosis
Amyloidosis - primary; Immunoglobulin light chain amyloidosis; Primary systemic amyloidosis; Primary localized amyloidosis
Primary amyloidosis is a rare disorder in which abnormal proteins build up in tissues and organs. Clumps of the abnormal proteins are called amyloid deposits.
Images

I Would Like to Learn About:
Causes
The cause of primary amyloidosis is not well understood. Genes may play a role.
The condition is related to abnormal and excess production of specific proteins. The proteins build up in certain organs. This makes it harder for the organs to work correctly.
Primary amyloidosis can lead to conditions that include:
- Carpal tunnel syndrome (due to protein deposits in the nerve)
- Heart muscle damage (cardiomyopathy) leading to congestive heart failure
- Intestinal malabsorption
- Liver swelling and malfunction
- Kidney failure
- Nephrotic syndrome (a group of signs that includes protein in the urine, low protein levels in the blood, high cholesterol levels, high triglyceride levels, and swelling throughout the body)
- Nerve problems (neuropathy)
- Orthostatic hypotension (drop in blood pressure when you stand up)
Symptoms
Symptoms depend on the organs affected. This disease can affect many organs and tissues, including the tongue, intestines, skeletal and smooth muscles, nerves, skin, ligaments, heart, liver, spleen, kidneys, and bladder.
Symptoms may include any of the following:
- Abnormal heart rhythm
- Fatigue
- Numbness of hands or feet
- Shortness of breath
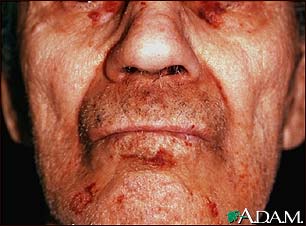
- Skin changes
- Swallowing problems
- Swelling in the arms and legs
- Swollen tongue
- Weak hand grip
- Weight loss or weight gain
Other symptoms that may occur with this disease:
- Decreased urine output
- Diarrhea
- Hoarseness or changing voice
- Joint pain
- Weakness
Exams and Tests
Your health care provider will examine you. You will be asked about your medical history and symptoms. A physical exam may show that you have a swollen liver or spleen, or signs of heart or nerve damage.
The first step in diagnosing amyloidosis should be blood and urine tests to look for abnormal proteins.
Other tests depend on your symptoms and the organ that may be affected. Some tests include:
- Abdominal ultrasound to check the liver and spleen
- Heart tests, such as an ECG, echocardiogram, or MRI
- Kidney function tests to check for signs of kidney damage (nephrotic syndrome or renal insufficiency)
Tests that can help confirm the diagnosis include:
- Abdominal fat pad aspiration
- Bone marrow biopsy
- Heart muscle biopsy
- Rectal mucosa biopsy
Treatment
Treatment may include:
- Chemotherapy
- Stem cell transplant
- Organ transplant
If the condition is caused by another disease (secondary amyloidosis), that disease should be aggressively treated. This may improve symptoms or slow the disease from getting worse. Complications such as heart failure, kidney failure, and other problems can sometimes be treated, when needed.
Outlook (Prognosis)
How well you do depends on which organs are affected. Heart and kidney involvement may lead to organ failure and death. Body-wide (systemic) amyloidosis can lead to death within 2 years.
When to Contact a Medical Professional
Contact your provider if you have symptoms of this disease. Also call if you have been diagnosed with this disease and have:
- Decreased urination
- Difficulty breathing
- Swelling of the ankles or other body parts that does not go away
Prevention
There is no known prevention for primary amyloidosis.
Related Information
CardiomyopathyAcute kidney failure
Carpal tunnel syndrome
Malabsorption
Endocrine glands
Respiratory
References
Buxbaum JN. The systemic amyloidoses. In: Hochberg MC, Gravallese EM, Smolen JS, van der Hejide D, Weinblatt ME, Weisman MH, eds. Rheumatology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 177.
Gertz MA, Dispenzieri A. Amyloidosis. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 174.
Gertz MA, Buadi FK, Lacy MQ, Hayman SR. Immunoglobulin light-chain amyloidosis (primary amyloidosis). In: Hoffman R, Benz EJ, Silberstein LE, et al, eds. Hematology: Basic Principles and Practice. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 93.
BACK TO TOPReview Date: 1/1/2025
Reviewed By: Frank D. Brodkey, MD, FCCM, Associate Professor, Section of Pulmonary and Critical Care Medicine, University of Wisconsin School of Medicine and Public Health, Madison, WI. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
![]()