

Health Library
Multiple endocrine neoplasia (MEN) I
Wermer syndrome; MEN I
Multiple endocrine neoplasia (MEN) type I is a syndrome in which one or more of the endocrine glands are overactive or form a tumor. It is passed down through families.
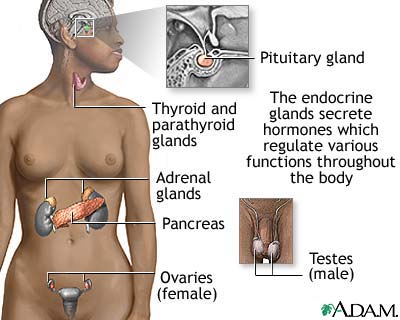
The endocrine glands most commonly involved are:
- Pancreas (islet cells)
- Parathyroid
- Pituitary
Images
I Would Like to Learn About:
Causes
MEN I is caused by a change in a gene that carries the code for a protein called menin. The condition causes tumors of various glands to appear in the same person, but not necessarily at the same time.
The disorder may occur at any age, and it affects men and women equally. A family history of this disorder raises your risk.
Symptoms
Symptoms vary from person to person, and depend on which gland is involved. They may include:
- Abdominal pain
- Anxiety
- Black, tarry stools
- Bloated feeling after meals
- Burning, aching, or hunger discomfort in the upper abdomen or lower chest that is relieved by antacids, milk, or food
- Decreased sexual interest
- Fatigue
- Headache
- Lack of menstrual periods (in women)
- Loss of appetite
- Loss of body or facial hair (in men)
- Mental changes or confusion
- Muscle pain
- Nausea and vomiting
- Sensitivity to the cold
- Unintentional weight loss
- Vision problems
- Weakness
Exams and Tests
Your health care provider will perform a physical exam and ask questions about your medical history and symptoms. The following tests may be done:
- Blood cortisol level
- CT scan of the abdomen
- Fasting blood sugar
- Genetic testing
- MRI of the abdomen
- MRI of the head (pituitary)
- Serum adrenocorticotropic hormone
- Serum calcium
- Serum follicle stimulating hormone
- Serum gastrin
- Serum glucagon
- Serum insulin level
- Serum luteinizing hormone
- Serum parathyroid hormone
- Serum prolactin
- Serum thyroid stimulating hormone
- Ultrasound of the neck
Treatment
Surgery to remove the diseased gland is often the treatment of choice. Medicines such as cabergoline and bromocriptine may be used instead of surgery for pituitary tumors that release the hormone prolactin.
The parathyroid glands, which regulate calcium production, can be removed. However, it is difficult for the body to regulate calcium levels without these glands, so a total parathyroid removal is not done first in most cases.
Medicines are available to decrease the excess stomach acid production caused by some tumors (gastrinomas), and to reduce the risk of ulcers.
Hormone replacement therapy is given when entire glands are removed or do not produce enough hormones.
Outlook (Prognosis)
Pituitary and parathyroid tumors are usually noncancerous (benign), but some pancreatic tumors may become cancerous (malignant) and spread to the liver. These can lower life expectancy.
The symptoms of peptic ulcer disease, low blood sugar, excess calcium in the blood, and pituitary dysfunction usually respond well to appropriate treatment.
Possible Complications
The tumors can keep coming back. Symptoms and complications depend on which glands are involved. Regular check-ups by your provider are essential.
When to Contact a Medical Professional
Contact your provider if you notice symptoms of MEN I or have a family history of this condition.
Prevention
Screening close relatives of people affected with this disorder is recommended.
Related Information
Peptic ulcerLow blood sugar
Kidney stones
Pituitary tumor
Zollinger-Ellison syndrome
Parathyroid cancer
References
National Comprehensive Cancer Network website. Clinical practice guidelines in oncology (NCCN guidelines): neuroendocrine and adrenal tumors. Version 3.2025. www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf. Updated October 1, 2025. Accessed February 23, 2026.
Newey PJ, Thakker RV. Endocrine neoplasia syndromes. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15th ed. Philadelphia, PA: Elsevier; 2025:chap 42.
Newey PJ, Thakker RV. Multiple endocrine neoplasia type 1. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 133.
Nieman LK, Spiegel AM. Polyglandular disorders. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 212.
BACK TO TOPReview Date: 1/25/2026
Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language.
© 1997-
2026 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures.
![]()