

Health Library
Addison disease
Adrenocortical hypofunction; Chronic adrenocortical insufficiency; Primary adrenal insufficiency; Addison's disease
Addison disease is a disorder that causes the adrenal glands to not produce enough hormones.
Images
I Would Like to Learn About:
Causes
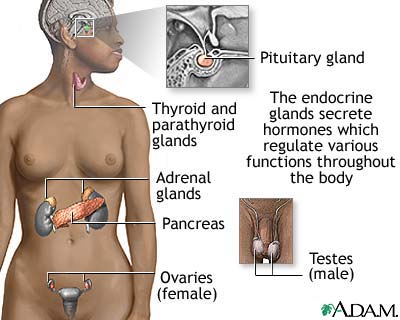
The adrenal glands are small hormone-releasing organs located on top of each kidney. They are made up of an outer portion, called the cortex, and an inner portion, called the medulla.
The cortex produces 3 hormones:
- Glucocorticoid hormones (such as cortisol) maintain sugar (glucose) control, blood pressure, decrease (suppress) immune response, and help the body respond to stress.
- Mineralocorticoid hormones (such as aldosterone) regulate sodium, water and potassium balance.
- Sex hormones, androgens (male) and estrogens (female), affect sexual development and sex drive.
Addison disease results from damage to the adrenal cortex. The damage causes the cortex to produce hormone levels that are too low.
This damage may be caused by the following:
- The immune system mistakenly attacking the adrenal glands (autoimmune disease)
- Infections such as tuberculosis, HIV, or fungal infections
- Hemorrhage into the adrenal glands
- Tumors
Risk factors for the autoimmune type of Addison disease include other autoimmune diseases:
- Swelling (inflammation) of the thyroid gland that often results in reduced thyroid function (chronic thyroiditis)
- Thyroid gland produces too much thyroid hormone (overactive thyroid, Graves disease)
- Itchy rash with bumps and blisters (dermatitis herpetiformis)
- Parathyroid glands in the neck do not produce enough parathyroid hormone (hypoparathyroidism)
- Pituitary gland does not produce normal amounts of some or all of its hormones (hypopituitarism)
- Autoimmune disorder that affects the nerves and the muscles they control (myasthenia gravis)
- Body does not have enough healthy red blood cells (pernicious anemia)
- Testicles cannot produce sperm or male hormones (testicular failure also called male hypogonadism)
- Type I diabetes
- Loss of brown color (pigment) from areas of the skin (vitiligo)
Certain rare genetic defects may also cause adrenal insufficiency.
Symptoms
Symptoms of Addison disease may include any of the following:
- Abdominal pain
- Chronic diarrhea, nausea, and vomiting
- Darkening of the skin
- Dehydration
- Dizziness when standing up
- Low-grade fever
- Low blood sugar
- Low blood pressure, especially with a change in body position
- Extreme weakness, fatigue, and slow, sluggish movement
- Darker skin on the inside of the cheeks and lips (buccal mucosa)
- Salt craving (eating food with a lot of added salt)
- Weight loss with reduced appetite
Symptoms may not be present all the time. Many people have some or all of these symptoms when they have an infection or other stress on the body. Other times, they have no symptoms.
Exams and Tests
Your health care provider will perform a physical exam and ask about your symptoms.
Blood tests will likely be ordered and may show:
- Increased potassium
- Low cortisol level
- Low sodium level
- Low pH
- Normal testosterone and estrogen levels, but low DHEA level
- High eosinophil count
Additional lab tests may be ordered.
Other tests may include:
Treatment
Treatment with replacement corticosteroids and mineralocorticoids will control the symptoms of this disease. These medicines usually need to be taken for life.
Never skip doses of your medicine for this condition because life-threatening reactions may occur.
Your provider may tell you to increase your dosage for a short time because of:
- Infection
- Injury
- Stress
- Surgery
During an extreme form of adrenal insufficiency, called adrenal crisis, you must inject hydrocortisone right away. Treatment for low blood pressure is usually needed as well.
Some people with Addison disease (or family members) are taught to give themselves an emergency injection of hydrocortisone during stressful situations. Always carry medical ID (card, bracelet, or necklace) that says you have adrenal insufficiency. The ID should also say the type of medicine and dosage you need in case of an emergency.
Outlook (Prognosis)
With hormone therapy, many people with Addison disease are able to lead a nearly normal life.
Possible Complications
Complications can occur if you take too little or too much adrenal hormone.
When to Contact a Medical Professional
Contact your provider if:
- You are unable to keep your medicine down due to vomiting.
- You have stress such as infection, injury, trauma, or dehydration. You may need to have your medicine adjusted.
- Your weight increases over time.
- Your ankles begin to swell.
- You develop new symptoms.
- While taking treatment, you develop signs of a disorder called Cushing syndrome
If you have symptoms of adrenal crisis, give yourself an emergency injection of your prescribed medicine. If it is not available, go to the nearest emergency room or call 911 or the local emergency number.
Symptoms of adrenal crisis include:
- Abdominal pain
- Difficulty breathing
- Dizziness or lightheadedness
- Low blood pressure
- Reduced level of consciousness
Related Information
Adrenal glandsImmune response
Pulmonary tuberculosis
Autoimmune diseases
Type 1 diabetes
Hypoparathyroidism
Hypopituitarism
Pernicious anemia
Graves disease
Chronic thyroiditis (Hashimoto disease)
Thrush - children and adults
Dermatitis herpetiformis
Vitiligo
Myasthenia gravis
Diabetes
Hyperthyroidism
Premature ovarian failure
Male hypogonadism
References
Auchus RJ, Pandey CEF. The adrenal cortex. In: Melmed S, Auchus RJ, Goldfine AB, Rosen CJ, Kopp PA, eds. Williams Textbook of Endocrinology. 15h ed. Philadelphia, PA: Elsevier; 2025:chap 13.
Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. PMID: 26760044 pubmed.ncbi.nlm.nih.gov/26760044/.
Nieman LK. Adrenal cortex. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 208.
BACK TO TOPReview Date: 4/24/2025
Reviewed By: Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 | A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complies with the HONcode standard for trustworthy health information: verify here. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language.
© 1997-
2026 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
All content on this site including text, images, graphics, audio, video, data, metadata, and compilations is protected by copyright and other intellectual property laws. You may view the content for personal, noncommercial use. Any other use requires prior written consent from Ebix. You may not copy, reproduce, distribute, transmit, display, publish, reverse-engineer, adapt, modify, store beyond ordinary browser caching, index, mine, scrape, or create derivative works from this content. You may not use automated tools to access or extract content, including to create embeddings, vectors, datasets, or indexes for retrieval systems. Use of any content for training, fine-tuning, calibrating, testing, evaluating, or improving AI systems of any kind is prohibited without express written consent. This includes large language models, machine learning models, neural networks, generative systems, retrieval-augmented systems, and any software that ingests content to produce outputs. Any unauthorized use of the content including AI-related use is a violation of our rights and may result in legal action, damages, and statutory penalties to the fullest extent permitted by law. Ebix reserves the right to enforce its rights through legal, technological, and contractual measures.
![]()